2015 Legacy - The diagnosis
A prototype that changed the organization’s direction
How native AI made the original thesis fully executable — and what care orchestration looks like when the technology can finally carry the burden
My Role
Sr. UX Strategist
Organization
Oracle Health
Year
2024
Artifacts
Presentation
This work is available for a deeper walkthrough — reach out to schedule a conversation.
The problem
Within the same enterprise application, nurses and physicians were working in incompatible experiences
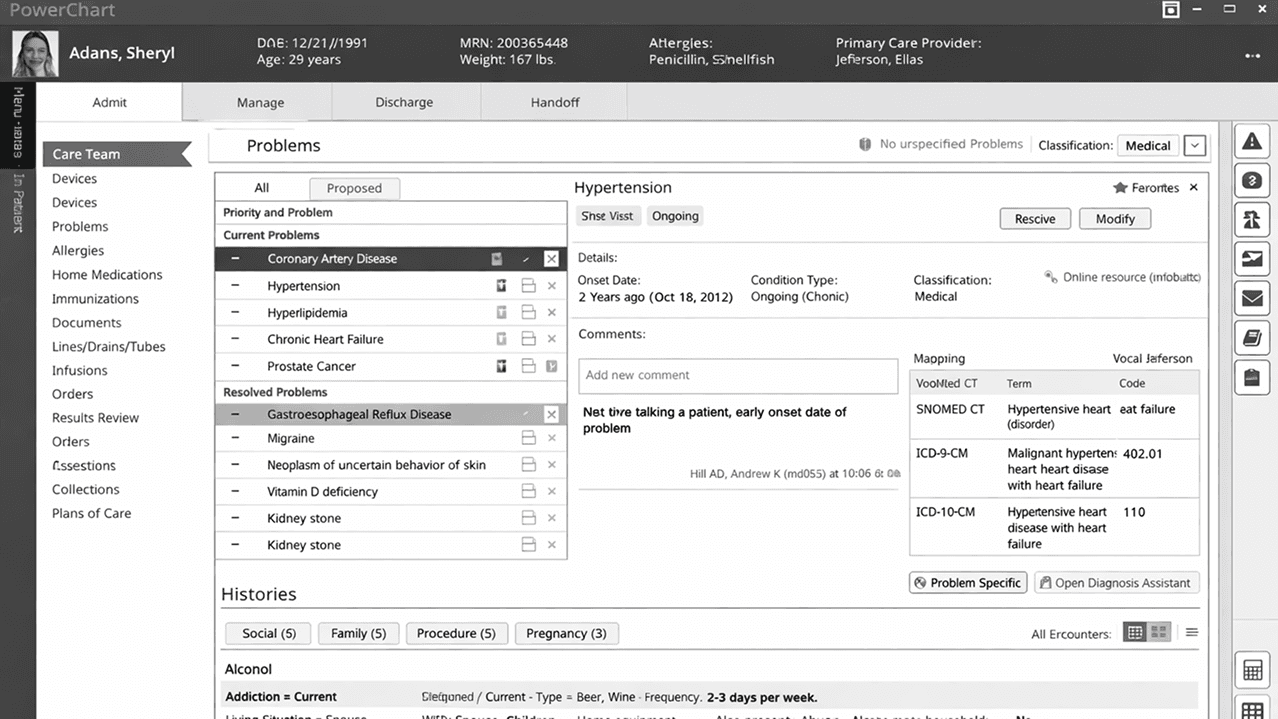
Cerner's PowerChart was a single enterprise application serving both physicians and nurses — but inside that application, the experiences were entirely disconnected. Physicians had access to a modern interface with updated components and interaction patterns. Nursing UIs were siloed, inconsistent with what physicians were using, and built without the shared capabilities that the physician experience had introduced.
The result was a fractured care team. Two clinicians responsible for the same patient, working inside the same application, couldn't collaborate effectively because they were looking at different displays and interacting with different systems of components. The fragmentation wasn't across platforms — it was structural, built into the architecture of the product itself.
This wasn't a feature gap. It was a foundational design failure. The enterprise application had grown role by role without a unifying framework, and the cost was paid by every care team trying to coordinate around a patient.
My contribution
I built a working prototype that showed what a unified experience could look like
Rather than writing a requirements document or a research report, I built a working HTML prototype. It demonstrated nurses operating within the same MPage interface as physicians — the same components, the same information architecture, the same visual language. If a nurse and physician were in the room together, they could be anchored to the same display and speak from the same picture of the patient.
The prototype introduced two concepts that would shape the platform for years. First, it organized the clinical experience into distinct phases of patient work — representing different stages of the encounter as discrete contexts rather than a single undifferentiated screen. Second, it introduced a persistent panel on the side of the interface: a zone for omnipresent capabilities that stayed accessible regardless of where the clinician was in their workflow.
That persistent panel was the origin of what would become the Situation Awareness and Notifications zone in Gen 1 Refined — and the Action Panel in Gen 2.
What happened
The demo didn’t just get approved — it redirected the organization
The reaction from clinicians and executive leadership was immediate. The nursing product lead championed the concept through approvals, and the work launched within the year. But the impact extended well beyond the nursing workstream.
When the broader UX team and product management saw what a working prototype could do — how it could communicate a vision that no slide deck or specification could — they adopted the approach. The demo became a method. The organization's model for how UX influenced product direction shifted as a result, with the full clinical suite becoming the subject of a coordinated reimagination.
Outcomes
Nursing and physician workflows unified into a shared interface framework within PowerChart, enabling real-time clinical collaboration
Work launched within the same year, championed by clinical product management leadership
Prototype-led strategy adopted across the UX organization, triggering a reimagination of the full clinical suite
Persistent panel concept originated here became the platform’s Situation Awareness zone and ultimately Gen 2’s Action Panel — independently validated a decade later by a team with no knowledge of the original concept
This is the first chapter of a decade-long argument. The unified interface solved the immediate collaboration problem — but it also surfaced something larger: the platform had no coherent model for how clinical information should be organized, prioritized, or delivered. That became the work of the next three years.