DESIGN THESIS
The EHR was built to
document care.
Not to support it.
My design instinct has always oriented toward the same question: where is the system asking humans to carry a burden that the technology should be carrying instead? That question is what connects everything in this portfolio.
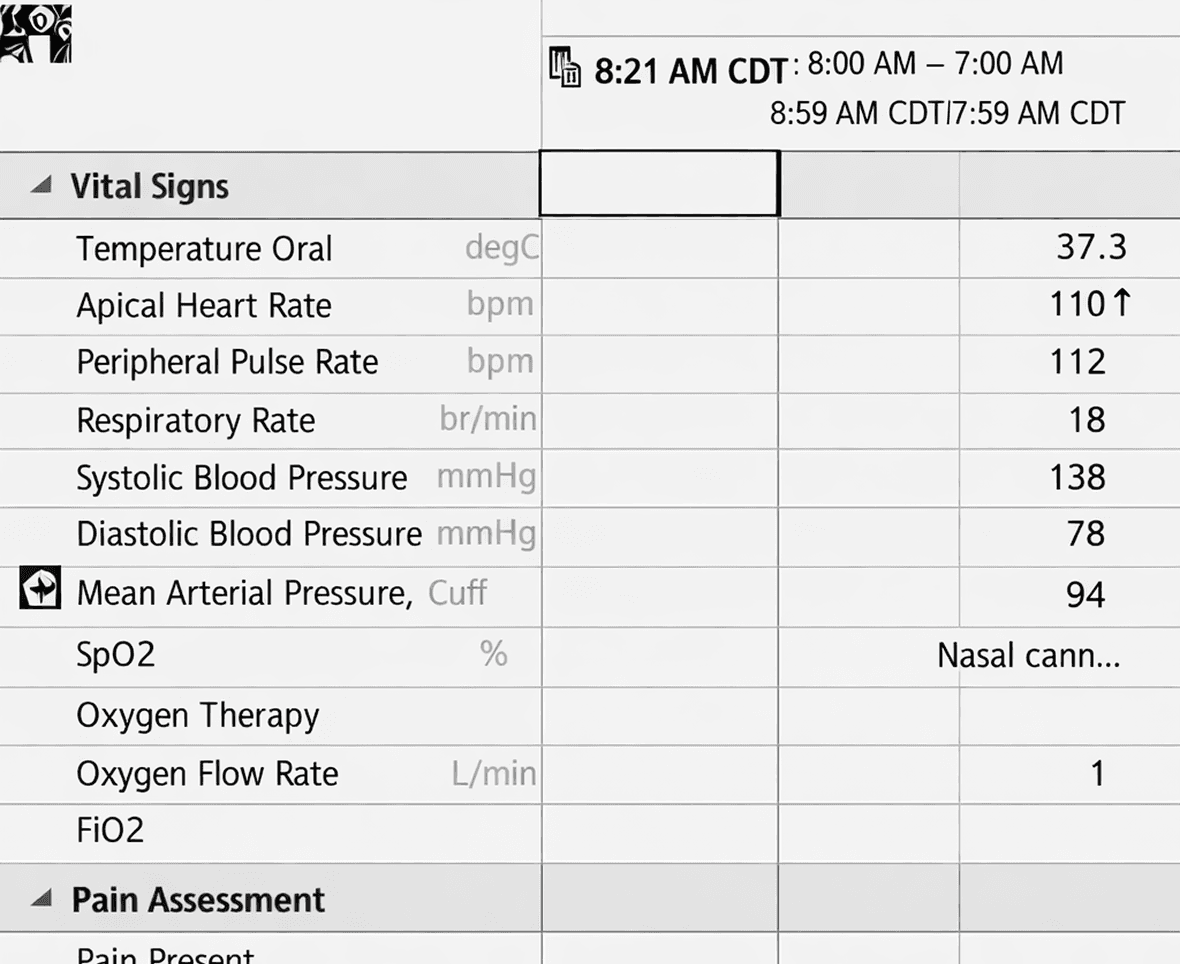
By the time I started leading clinical UX strategy at Cerner in 2013, the evidence was already accumulating. Physicians were spending nearly twice as much time interacting with the system as with patients. Nurses were working in fragmented interfaces that made collaboration with physicians nearly impossible. The electronic health record had met every regulatory requirement and failed nearly every clinical one.
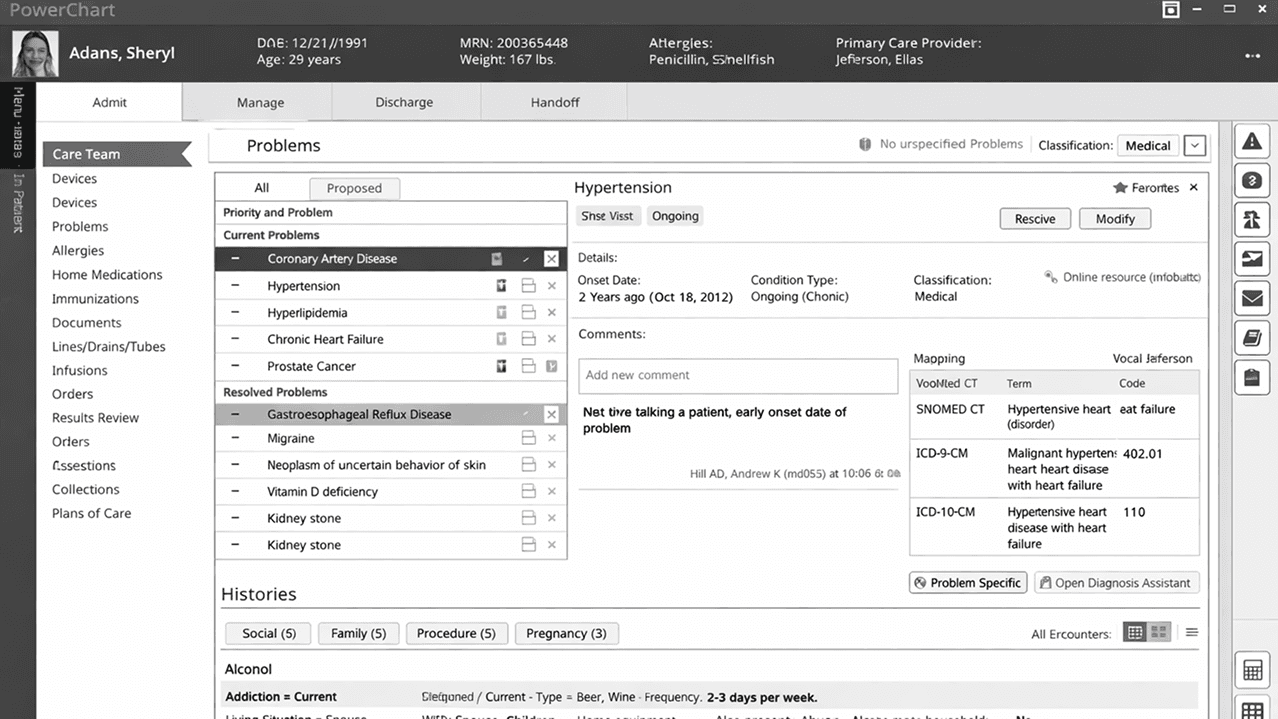
The root problem wasn’t usability. It was architecture. The system had been designed as a data repository and the clinician was expected to be the intelligence layer. They had to forage for information — locating it, retrieving it, assembling it, interpreting it — every time, for every patient, at every stage of care. All of the cognitive work the system should have been doing was being offloaded onto the people least able to afford the distraction.
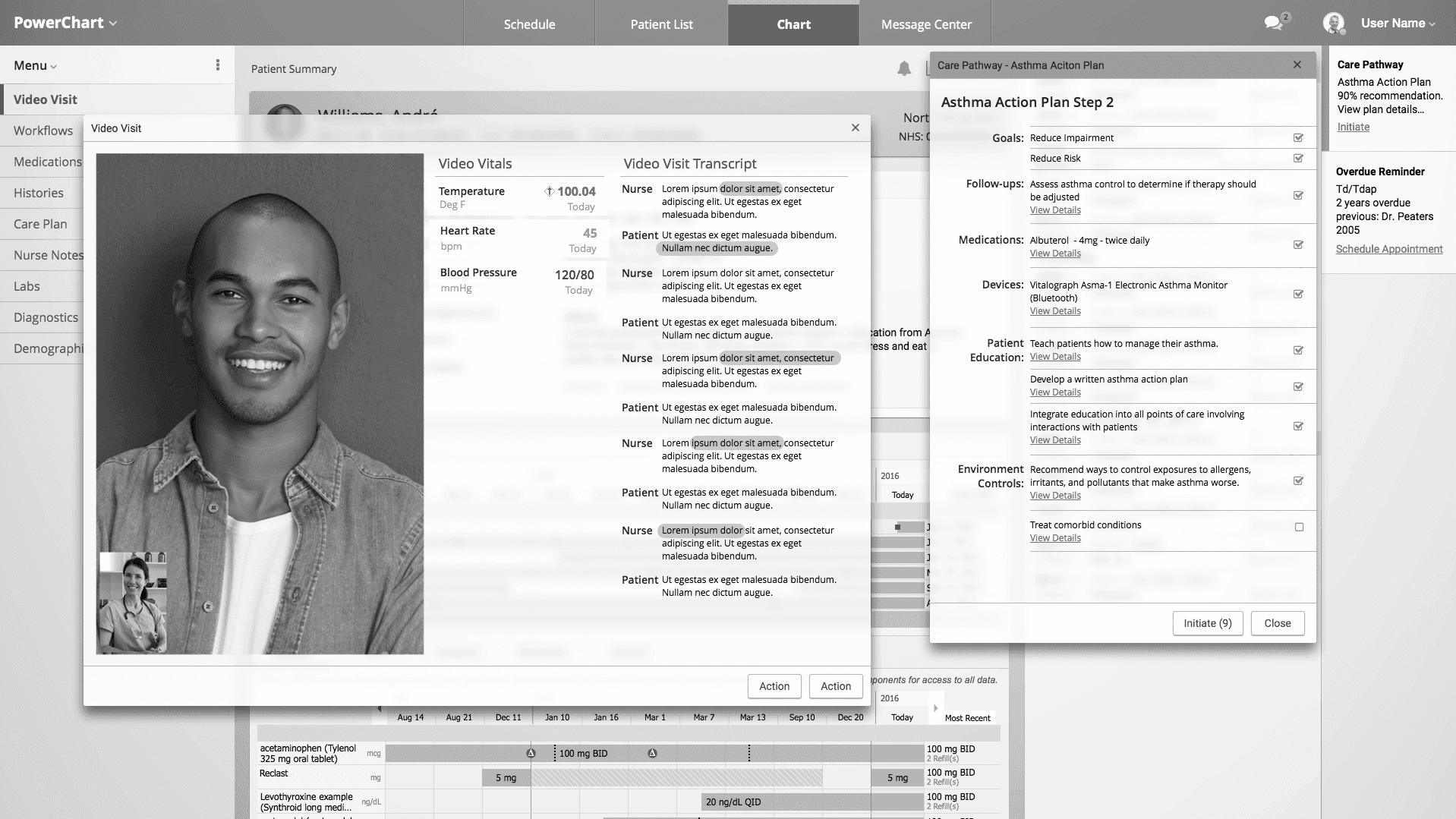
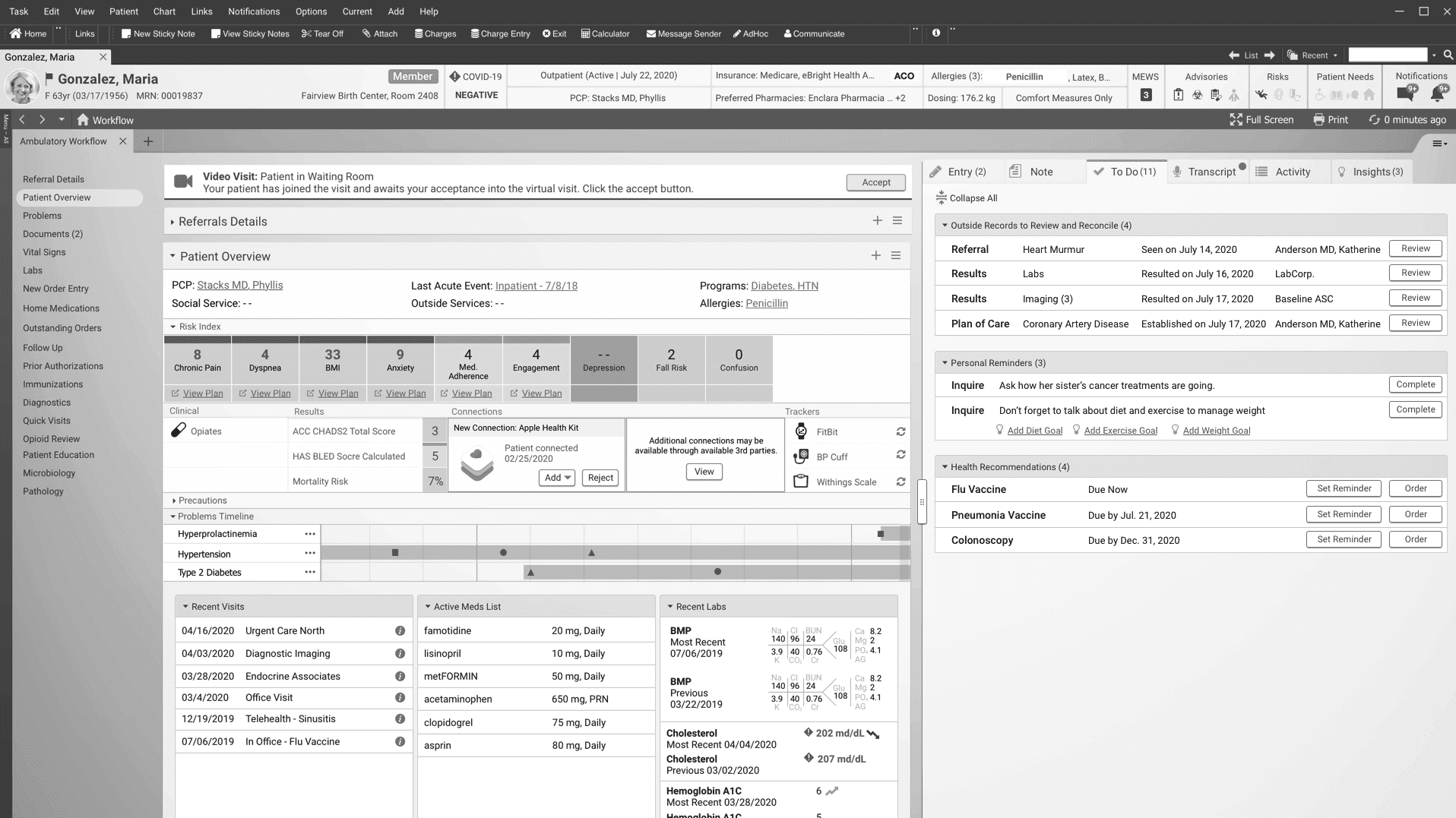
My work over the next decade was aimed at inverting that relationship. Technology should carry the burden. The system should know where the clinician is in the care cycle, what they need to know, and when they need to know it — so they can focus on the person in front of them.
2015 — Legacy
The diagnosis
Fragmented interfaces, siloed roles, and no shared clinical framework. A prototype changed the organization's direction.
Read the case study
2018 — Legacy
The pivot
Multi-site research made the failure undeniable. A demonstrated vision became the organization's strategic direction.
Read the case study
2020 — Legacy
The validation
A unified cross-continuum experience presented to the Board of Directors as the platform's go-forward vision.
Read the case study
2024 — Modernization
The fulfillment
Native AI makes the original thesis fully executable. The system finally becomes the intelligence layer.
Read the case study
The most important design problem in healthcare technology isn’t how information is displayed — it’s who is expected to do the work of making sense of it.
THE RESEARCH THAT SUPPORTS THIS
This thesis isn’t intuition. It is independently supported by a decade of peer-reviewed literature in human factors, biomedical informatics, and clinical workflow research. The problem was real, documented, and consequential — and the direction of the solution was already visible in the evidence.
THE THEORETICAL FOUNDATION - INFORMATION FORAGING THEORY
Pirolli and Card, 1999 (Psychological Review) — established that people navigate information environments the way animals forage for food, following information scent and making cost-benefit decisions about where to search. The EHR problem is a classic foraging failure: weak scent, high navigation cost, fragmented information patches that force repeated retrieval trips. The word “forage” in this portfolio is not a metaphor. It is a precise theoretical term.
Ash, Berg & Coiera · JAMIA · 2004
EHR design created new cognitive burdens it was supposed to reduce
Documented unintended adverse consequences of health IT — workflow interruptions, information fragmentation, and cognitive load that increased rather than decreased with system adoption.
Shanafelt et al. · Mayo Clinic Proceedings · 2016
Clinicians spent nearly twice as much time on the EHR as with patients
Ambulatory physicians averaged 49.2% of office time on EHR and desk work versus 27% face-to-face with patients — a quantitative measure of how completely the system had displaced the person.
Melnick et al. · Annals of Family Medicine · 2017
Worse EHR usability directly predicted higher clinician burnout
Connected interface quality to clinician harm — establishing that this was not an inconvenience problem but a measurable health and safety issue for the care workforce.
Topol · The Lancet · 2019
AI in healthcare should restore the human connection, not extend screen time
Argued that the purpose of AI in medicine is to give clinicians back the time and attention the EHR took from them — framing intelligent systems as a restoration of the clinician-patient relationship.
THE SOLUTION FRAMEWORK
Endsley, 1988 and 1995 — defined Situation Awareness as perception of current state, comprehension of its meaning, and projection of what may occur. A contextually intelligent clinical system must support all three levels across the full arc of the encounter: before entering the room, during the visit, and between encounters. This framework became the theoretical backbone of the workspace architecture and notification philosophy developed across Gen 1 and Gen 1 Refined.
A critical design consideration for AI in healthcare
AI that requires a conversation is still a computer between the clinician and the patient
The current wave of AI in healthcare introduces a risk the field hasn’t fully reckoned with. Many implementations take a conversational or bolt-on approach — a chat interface, a prompted assistant, a wake word the clinician must use to invoke the system. The capability may be more powerful than what came before. But the interaction model repeats the original mistake.
If a clinician has to stop, open a panel, speak a trigger phrase, and wait for a response — the system is still the object of their attention. The computer is still between them and the patient. A smarter search box is still a search box.
The right model requires three things working together: ambient delivery, continuous learning, and contextual participation. Clinical AI needs to do all three simultaneously, in the background, without requiring the clinician to stop and engage.
01
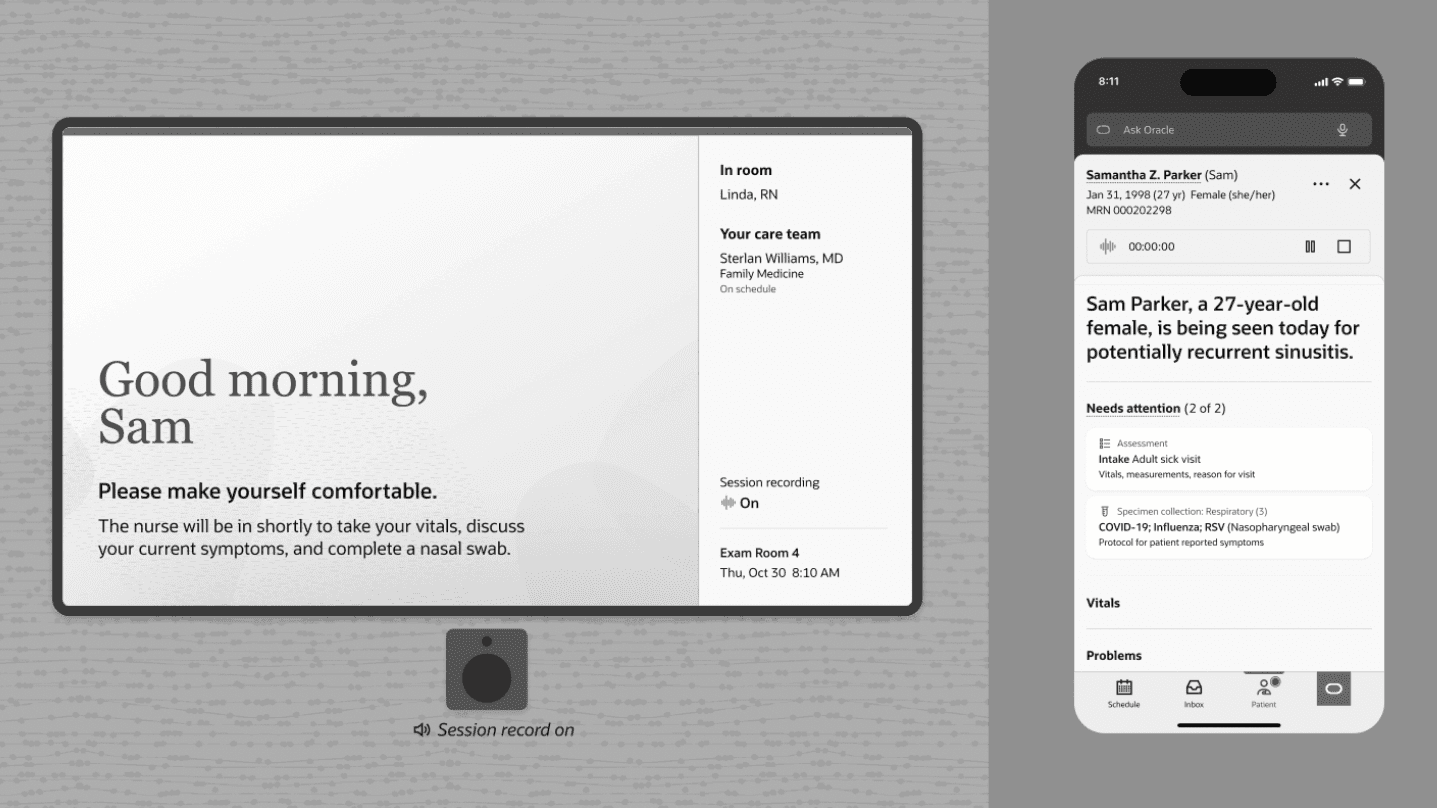
Ambient delivery
The system observes context and surfaces information without being asked. No wake word. No query. No interruption to workflow.
02
Continuous learning
The system builds understanding over time — across encounters, across patients, across clinician patterns. It gets better at knowing what matters without being retrained by the user.
03
Active participation
The system is a silent participant in the evolving clinical conversation. It doesn't wait to be called on. It maintains awareness of the situation and acts from that awareness at the right moment.
This maps directly to Endsley's three levels of Situation Awareness. Perception is the AI observing what's happening in real time. Comprehension is the AI building meaning from what it has observed across the encounter and over time. Projection is the AI anticipating what will likely be needed next — and delivering it before the clinician has to ask. That is not a query interface. That is a cognitive partner.
Conversational / bolt-on AI
Clinician must stop and invoke the system
Responds to prompts — does not participate
No persistent awareness between interactions
Computer remains the object of attention
Smarter tool — same structural problem
Ambient intelligence
Maintains awareness without being invoked
Active participant in the evolving clinical context
Learns continuously
Patient remains the object of attention
Different architecture — different outcome
The clinical safety dimension
A clinician who must invoke an AI to receive a warning may miss the window where that warning mattered. An AI that has been maintaining situational awareness throughout the encounter surfaces a concern at the moment it becomes clinically relevant — not when the clinician remembers to ask. The difference between those two models is not a user experience preference. In high-acuity settings, it is a patient safety distinction.