2024 Modernization : The fulfillment
The system finally becomes the intelligence layer
How native AI made the original thesis fully executable — and what care orchestration looks like when the technology can finally carry the burden
My Role
Sr. UX Strategist
Organization
Oracle Health
Year
2024
Artifacts
Presentation
This work is available for a deeper walkthrough — reach out to schedule a conversation.
The context
Oracle’s native AI created the conditions the thesis had always required
The argument had been building for a decade. EHRs were designed as data repositories and clinicians were expected to be the intelligence layer — locating, retrieving, assembling, and interpreting information at every step of every encounter. The research was unambiguous. The design direction was clear. What had been missing was the technology to fully execute it.
Oracle Health’s native AI capabilities changed that. For the first time, the system could do the cognitive work that had always been offloaded onto clinicians. It could pull fragmented data into coherent context before anyone asked. It could listen, learn, and document in real time. It could surface the right information at the right moment through the right channel — without requiring the clinician to navigate to it.
In Gen 2, I served as the domain expert for the broader design team while leading the nursing experience specifically. My influence is present across the platform's clinical direction. My deliverable was Care in Motion — the most complex version of the original problem, applied to nursing workflow across the full arc of a patient encounter.
The problem
Care orchestration is the hardest unsolved problem in healthcare UX
Care orchestration spans the entire patient journey — from scheduling through post-visit follow-through — across multiple roles, systems, and venues. Three distinct failure points define where it breaks down.
Before the encounter, interoperability failures mean that information relevant to the patient exists across multiple systems and the clinician has no reliable way to pull it together. The cognitive work of assembling context falls entirely on the care team.
During the encounter, coordination between patient, nurse, and physician requires constant back-and-forth task management with no shared orchestration layer. Who does what, in what order, gets managed informally — through conversation, memory, and manual tracking.
After the encounter, the thread breaks. Referrals go unconfirmed. Patient action items don't communicate back to clinicians. The system loses awareness of the patient the moment they walk out the door.
Care in motion
Every moment in the nursing workflow, the system knows what’s needed and surfaces it
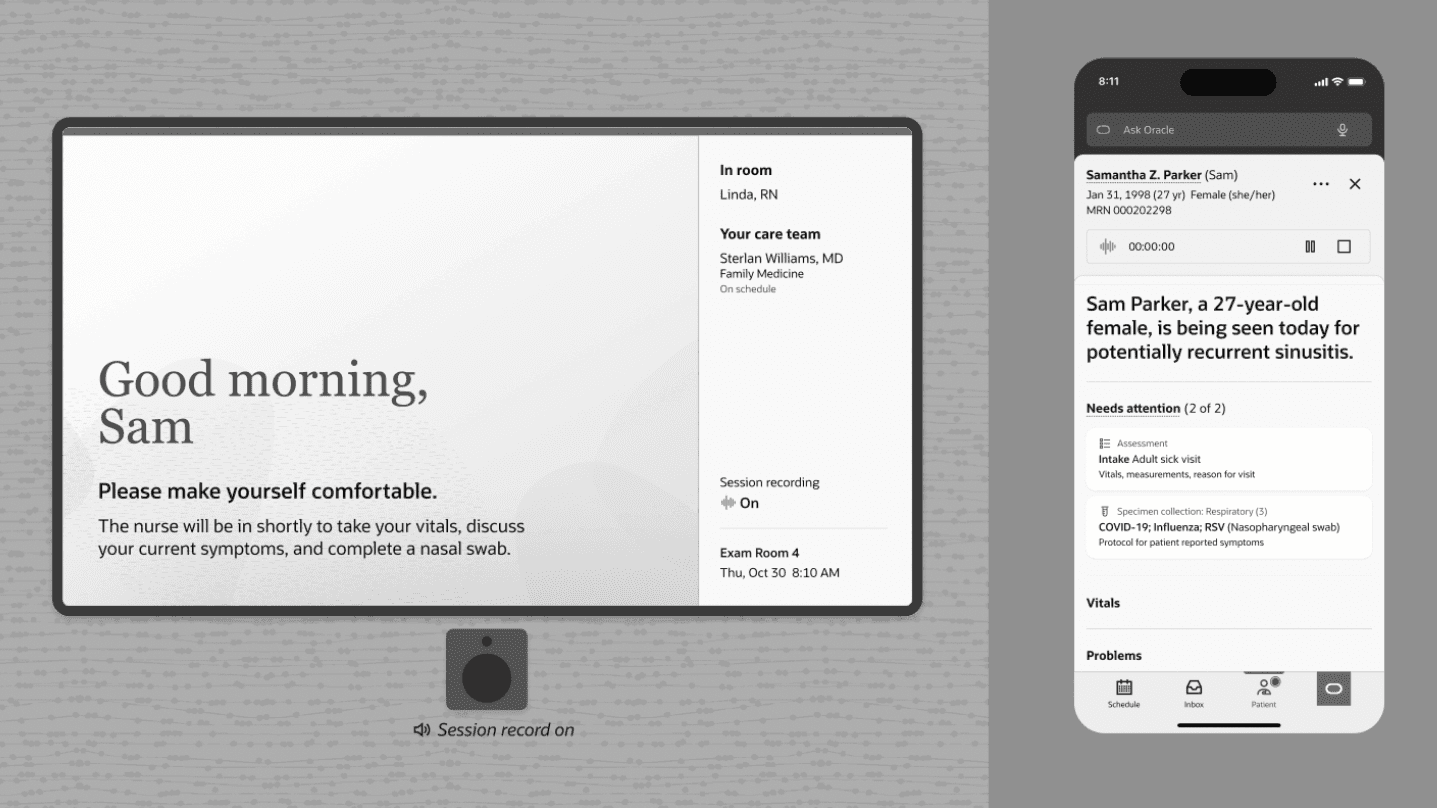
Care in Motion demonstrates the thesis at full resolution. The nursing experience follows Nurse Linda and patient Sam through a complete ambulatory encounter — from Sam’s initial AI-assisted scheduling call through Linda’s afternoon phone triage. At no point does Linda have to forage for information. The system carries it to her.
Where the system carries the burden — key moments from Care in Motion
Scene 1
AI schedules the appointment
Sam calls with symptoms. An AI scheduling assistant understands her situation and books on her behalf. Her only job is to rest.
Scene 3
Linda gets oriented before the day begins
A dynamic, role-specific schedule gives Linda a bird’s-eye view and the ability to drill into detail. She’s prepared before stepping into the clinic huddle.
Scene 6
Bird’s-eye view surfaces what Linda needs to know
A dynamic, role-specific schedule gives Linda a bird’s-eye view and the ability to drill into detail. She’s prepared before stepping into the clinic huddle.
Scene 7
Ambient listening handles documentation
With Sam’s consent, ambient listening documents the conversation in real-time — adding new symptoms, updating the family history, confirming medication lists. Linda focuses on Sam, not the screen.
Scene 8
Earpiece notification with contextual summary
A priority notification in Linda’s earpiece tells her Gracie has checked in, summarizes her situation, and recommends an accessible room. Linda acts — she doesn’t research.
Scene 10
Phone triage with AI-assembled context
An 85-year-old patient's son calls about an ED visit. The system has already pulled the patient’s last visit, the ED discharge summary, and recommended next steps. Linda follows protocol — she doesn’t forage.
Independent convergence on the same architectural answer
In 2015, I prototyped a persistent panel concept — a zone for omnipresent capabilities that stayed accessible regardless of where the clinician was in their workflow. I was not involved in Gen 2's Action Panel development. The Gen 2 team arrived at the same architectural answer independently, driven by the same clinical needs. When two separate teams, a decade apart, solving the same problem, converge on the same structural solution without one influencing the other — the idea was right. The problem demanded that answer.
30%
Reduction in task completion time through AI-powered workflow optimization
25+
UX professionals supported as domain expert across the clinical platform
17
Pending patent co-inventions across the body of work
Care in Motion demonstrates the thesis at full resolution — every step of the nursing workflow supported by a system that anticipates needs, surfaces context, and closes the loop
AI-assisted documentation, intelligent task prioritization, and automated contextual summaries reduced task completion time by 30% while maintaining quality standards
Care orchestration demonstrated as solvable through ambient intelligence, contextual delivery, and closed-loop task management — though the broader industry challenge of disconnected systems across the healthcare landscape remains ongoing
Domain expertise provided across the full Gen 2 clinical platform, with strategic influence present across demos and design directions beyond the nursing workstream
The problem was identified in 2015. The research confirmed it in 2018. The vision was validated in the boardroom in 2020. In 2024, the technology arrived to make it fully real. Care in Motion is not the end of this argument — care orchestration remains one of healthcare's hardest problems, constrained less by design vision than by the fragmented systems landscape that no single platform can fully solve alone. But it is the most complete demonstration yet of what it looks like when the system finally carries the burden it was always supposed to carry.