2018 Legacy - The Pivot
From research finding
to organizational vision
How multi-site clinical research validated the thesis, defined the platform's design language, and produced a demonstrated vision the organization adopted as its strategic direction
My Role
Sr. UX Strategist
Organization
Cerner Corporation
Year
2015 - 2018
Artifacts
Presentation/Research
This work is available for a deeper walkthrough — reach out to schedule a conversation.
By 2018 the thesis had a name the whole organization was using. The research had been validated at scale. A working demonstration showed it was buildable. What remained was securing the organizational commitment and investment to build it at the platform level. That became the work of the next chapter.
The problem
The platform had met its regulatory obligations and failed its users
Meaningful Use compliance had been achieved. But across clinical research between 2015 and 2018, a different picture was emerging. Clinicians couldn’t understand the patient story from within the EHR. They had to go to multiple places to manually assemble information that should have been coherent and accessible. The order of clinical events mattered deeply to care decisions — and the system made that order nearly impossible to see.
External research was reaching the same conclusion. Studies showed physicians spending nearly twice as much time on EHR and desk work as with patients. After-hours documentation extended work into personal time. Worse EHR usability was directly linked to higher burnout rates. The system wasn't just inconvenient — it was measurably harming the people using it.
The root cause was architectural. The EHR had been designed as a data repository and the clinician was expected to be the intelligence layer. They had to forage for information every time, for every patient, at every stage of care. All of the cognitive work the system should have been doing was being offloaded entirely onto them.
The Research
Dozens of participants across multiple health systems. The same finding everywhere.
75
Clinicians and staff across all workshops
4
Health system sites, multiple care settings
7
Structured research sessions per site
Working with our Sr. Human Factors Researcher, I led a multi-site, multi-month research engagement spanning acute care settings across multiple health systems. Each site participated in full-day workshops of 12 to 35 clinicians, structured around seven sessions covering problem definition, use cases, data needs, goals, ideation, and success criteria.
Across every site and every care setting, the finding was the same. It was difficult to see the overall picture of a patient's visit. The order of events was important and not easy to identify. Clinicians had to go to many places to manually assemble the story. Reviewing the record was time-intensive — and that time cost was paid directly at the expense of patient care.
Grounded in Endsley's Situation Awareness framework — perception of current state, comprehension of its meaning, projection of what may occur — we translated these findings into a model for what a contextually intelligent clinical system needed to do.
The Vision
The research produced a demonstrated concept, not just a report
“Contextual and Intelligent Experiences: Supercharging our solutions to remove the cognitive burden from our end users”
Cerner 2018 — the organizational language that formalized the thesis
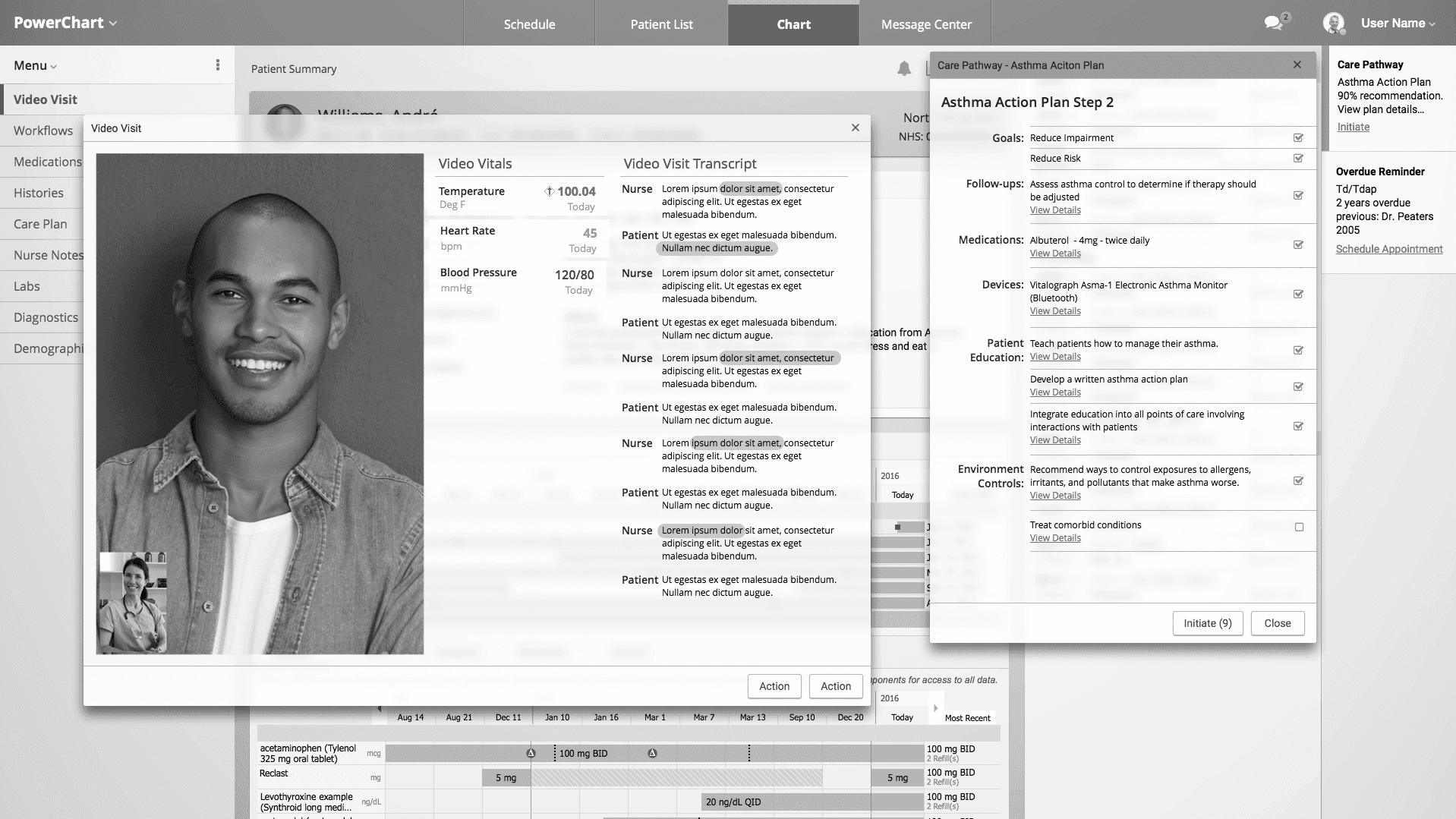
The research findings fed directly into a demonstrated vision I authored that showed what a contextually intelligent experience could look like across the full patient journey. The demo followed a single patient — André — from voice-activated AI scheduling through Alexa, through a video visit with real-time automated documentation, to smart device integration transmitting peak flow data directly to his chart, to an algorithm-triggered status escalation that notified his Care Manager through a Population Watch List.
Every moment in the demo answered the same question: where is the system carrying the burden so the clinician doesn't have to? By 2018 this framing — removing cognitive burden through contextual and intelligent design — became the organization's strategic language. My strategy work had not just identified the problem. It had shown what solving it looked like.
Patient side
Voice-activated AI scheduling
Alexa books the appointment based on symptoms, insurance, and preferences. Patient’s only job is to rest.
Clinical Side
Automated documentation
Video visit transcribed and processed in real-time. Care pathways surfaced contextually. Clinician focuses on patient.
Care management
Algorithm-triggered escalation
Peak flow meter data triggers status change. Care Manager notified via Population Watch List before patient deteriorates.
Parallel workstreams
Research drove architectural decisions across two major initiatives
Organizational Impact
Five platform directions shifted. One strategic framing adopted.
Notification philosophy — a platform-wide framework replacing ad hoc alert design with a principled, research-grounded model
Reinforced design standards — consistency reframed as a clinical safety issue, not a visual preference
Interface simplification — cognitive load reduction adopted as an explicit design priority across the clinical application
Clinical results display improvements — better information hierarchy to reduce manual interpretation burden
Interoperability interface improvements — design investment in the experiences where information crossed system boundaries
The research and strategy work became a reference point for other UX strategists across the clinical portfolio — shaping how parallel workstreams framed their own problems and design directions